Why is my blood sugar always high after lunch, even when I feel okay?
Postprandial spikes hide behind normal HbA1c numbers. How diabetes remote monitoring surfaces the after-lunch pattern that point-in-time visits miss.
Feeling fine after a meal is one of the least reliable signals in diabetes care. A person can sit down to lunch, eat what looks like a reasonable plate, feel completely normal an hour later, and still be running a blood glucose level well above the threshold that drives long-term complications. This gap between how someone feels and what their physiology is actually doing is the central problem that diabetes remote monitoring is built to close. For chronic care management teams and value-based care organizations, the after-lunch glucose spike is a useful lens on a much larger issue: the most clinically important data points happen between visits, not during them.
Among patients with type 2 diabetes and apparently good metabolic control, 38 percent had more than 40 percent of their post-prandial readings above 160 mg/dL, according to a study of 3,284 patients published in the analysis of post-prandial hyperglycaemia prevalence (Bonora et al., reported in Diabetologia).
Why diabetes remote monitoring catches what office visits miss
Postprandial hyperglycemia is the formal name for the after-lunch problem, and it is far more common than most quarterly check-ups would suggest. Research summarized from continuous glucose monitoring cohorts found that people with type 2 diabetes spend roughly 38 percent of the day above 10 mmol/L (180 mg/dL), and even those with an HbA1c under 7.0 percent spend about 24 percent of the day in hyperglycemia. The DIALECT-2 cohort analysis (van der Aart-van der Beek and colleagues, MDPI, 2020) confirmed that as overall control improves, the relative contribution of post-meal spikes to total hyperglycemia actually grows. In other words, the better the A1c looks on paper, the more the remaining risk hides in the hours after eating.
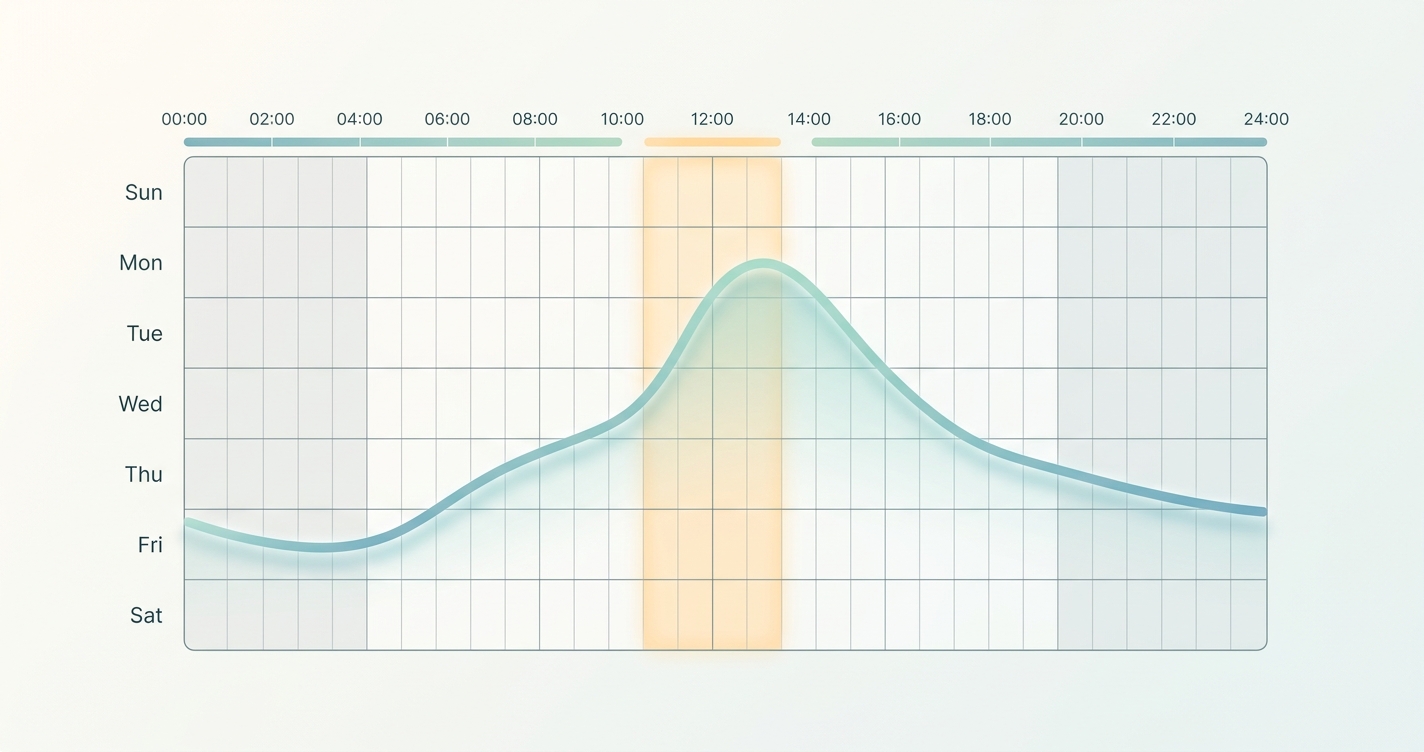
The reason a patient feels okay is simple physiology. Symptoms of high blood sugar, such as thirst, fatigue, or blurred vision, tend to appear at sustained levels far above the range where vascular damage accumulates. A glucose reading of 180 to 220 mg/dL after lunch rarely produces noticeable symptoms, yet it is exactly the kind of repeated excursion that compounds into retinopathy, neuropathy, and cardiovascular risk over years. A single fasting fingerstick at a morning appointment, or an A1c that averages everything into one number, cannot see this pattern at all.
This is the structural limitation that diabetes remote monitoring addresses. The clinical value is not any one reading. It is the ability to observe the same time of day, repeatedly, across normal life, and to notice that 1 p.m. is consistently a problem while 7 a.m. looks fine.
| Monitoring approach | What it captures | What it misses | Best fit |
|---|---|---|---|
| Quarterly office visit + A1c | A 3-month average, one fasting snapshot | Daily timing, meal-specific spikes, day-to-day variability | Baseline assessment, medication review |
| Episodic fingersticks | Discrete points the patient chooses to test | Untested windows, especially busy afternoons | Insulin titration in motivated patients |
| Continuous glucose sensors | Dense 24-hour glucose curve | Patients with device fatigue or cost barriers; non-glucose vitals | Insulin users, intensive management |
| Daily passive remote check-ins | Repeated patterns across many vitals over time | Minute-by-minute glucose resolution | Population-level CCM, trend detection |
What the after-lunch pattern tells a care team
When a care manager can see a recurring signal rather than a single value, the conversation changes. A patient who feels fine but shows a consistent midday excursion is not a candidate for alarm. They are a candidate for a small, specific adjustment. The pattern itself carries the information.
Useful patterns that only emerge from repeated daily observation include:
- A spike that appears after lunch but not breakfast, often pointing to a specific meal composition or portion habit
- Excursions that worsen on weekdays, suggesting a work-related eating or stress pattern
- Gradual upward drift across weeks, which may indicate medication losing effect or disease progression
- Post-meal highs paired with elevated resting heart rate or poor recovery, hinting at the broader metabolic strain that diabetes places on the cardiovascular system
None of these become visible from a number averaged over three months. They require frequency and consistency, which is the operational definition of diabetes remote monitoring done well.
Industry Applications
Chronic care management programs
For CCM teams managing large diabetes panels, the after-lunch question scales into a triage problem. Most patients do not need intervention on any given week, so the value of monitoring is its ability to separate stable patients from those whose patterns are shifting. Daily check-ins that require no device handling reduce the dropout that plagues many remote programs and keep the denominator of monitored patients high enough to be statistically meaningful.
Value-based care and ACOs
Organizations carrying financial risk for diabetes outcomes have a direct interest in catching deterioration early. A 2023 survey reported that 71 percent of type 2 diabetes patients favored remote monitoring for managing their health, up from 35 percent in 2021, which signals that patient acceptance is no longer the bottleneck. Remote monitoring programs have been associated with reduced avoidable admissions and emergency visits, the cost centers that value-based contracts are designed to control.
Primary care and endocrinology support
Between-visit data gives clinicians a reason to titrate medications based on observed behavior rather than a patient's recollection. When the data shows that lunch is the consistent problem, the intervention can be precise, whether that is a mealtime agent, a dietary change, or a timing adjustment, instead of a broad escalation that risks hypoglycemia.
Current research and evidence
The clinical case for richer between-visit data continues to build. A 2023 real-world observational study published in JMIR by Bergenstal-style digital health researchers found that combining continuous glucose data with a digital health solution improved Time in Range by roughly 15 percentage points for adults with type 2 diabetes, alongside a measurable drop in mean glucose. Broader reviews of remote patient monitoring report average HbA1c reductions near 0.55 percentage points compared with usual care, a difference large enough to matter at the population level.
The American Diabetes Association's Standards of Care in Diabetes 2023 formally recommended continuous glucose monitoring for people on insulin, and Medicare aligned its coverage criteria with those standards in April 2023, expanding access. These shifts reflect a wider recognition that point-in-time measurement is no longer the standard of evidence for chronic glycemic management. The prevalence data reinforces it: one analysis found post-prandial hyperglycemia in 73.5 percent of patients whose fasting glucose was controlled, meaning the "feel okay" patient is statistically the norm, not the exception.
What the research collectively shows is that the after-lunch spike is not an anomaly to be dismissed. It is a structural feature of type 2 diabetes that standard testing systematically underweights.
The Future of diabetes remote monitoring
The next phase is less about any single biomarker and more about combining signals. Glucose patterns are most informative when read alongside heart rate, heart rate variability, and respiratory trends, because diabetes rarely travels alone. The goal for chronic care programs is a low-friction stream of daily data that surfaces patterns without asking patients to manage hardware, replace sensors, or remember to test during a busy afternoon. Reducing device fatigue keeps more patients enrolled long enough for trends to mean something.
As reimbursement continues to reward outcomes over visit volume, the programs that win will be those that can show they detected the drift before it became a complication. The after-lunch spike is a small example of a large principle: in chronic disease, the signal lives in the repetition, and the organizations that can capture repetition cheaply and comfortably will define the next decade of chronic care.
Frequently asked questions
Why is my blood sugar high after lunch even when I feel fine? Symptoms of high blood sugar usually appear only at sustained, very elevated levels. A post-lunch reading of 180 to 220 mg/dL often causes no noticeable feeling but still contributes to long-term complications, which is why patterns matter more than how you feel.
Can an A1c test detect after-meal spikes? Not directly. An A1c reflects a roughly three-month average and cannot show what time of day your glucose rises. Post-prandial hyperglycemia frequently hides behind a normal-looking A1c, which is why repeated daily observation is more revealing.
How does diabetes remote monitoring help with this? Remote monitoring captures the same time of day repeatedly across normal life, allowing care teams to see that lunch is consistently a problem while other meals are not. That pattern guides precise, lower-risk adjustments.
Why do chronic care programs care about post-lunch patterns? For value-based care and ACO programs, recurring post-meal excursions are early markers of risk that, if caught, can prevent avoidable admissions and complications, the cost centers these programs are accountable for.
Circadify is building toward this future of low-friction, daily diabetes remote monitoring for chronic care management teams, using contactless check-ins that surface patterns without adding device burden. To see how a program like this fits a CCM or value-based care model, explore the chronic care management solution at circadify.com/solutions/chronic-care-management.